Bosniak renal cyst classification
The Bosniak classification system for CT evaluation of renal cysts is helpful in determining both malignant risk and required followup / treatment.
Bosniak 1
· simple cyst, anechoic, imperceptable wall, rounded
· work up : nil
· % malignant : ~ 0
Bosniak 2
· minimally complex, single thin (< 1mm) septations, thin Ca++; non-enhancing high-attenuation renal lesions of less than 3 cm are also included in this category; these lesions are generally well marginated.
· work up : nil
· % malignant : ~ 0
Bosniak 2F
· minimally complex but requiring follow up.
· increased number of septa, minimally thickened or enhancing septa or wall
· thick Ca++,
· hyperdense cyst that is:
o > 3 cm diameter, mostly intrarenal (less than 25% of wall visible); no enhancement
· work up : needs ultrasound / CT follow up
· % malignant : ~ 5 %
Bosniak 3
· indeterminate, thick or multiple septations, mural nodule, hyperdense on CT (see 2F)
· treatment / work up : partial nephrectomy or RF ablation in elderly / poor surgical risk
· % malignant : ~ 50%
Bosniak 4
· clearly malignant, solid mass with cystic spaces surgery
· treatment: partial / total nephrectomy
· % malignant : ~100%
Renal cell carcinoma staging
TNM staging
T
· T1
o T1a : limited to kidney < 4 cm
o T1b : limited to kidney > 4 cm, < 7 cm
· T2 : limited to kidney > 7 cm
· T3 : tumour / tumour thrombus extension into adrenal or renal vein or perinephric tissues (but contained by Gerota's fascia)
o T3a : spread to perinephric fat
o T3b : spread to renal vein or intra diaphragmatic IVC
o T3c : spread to supra diaphragmatic IVC
N
· N0 : no nodal involvement
· N1 : single regional lymph node involved
· N2 : beyond N1 (NB laterality does NOT affect nodal staging)
M
· M0 : no distant metastases
· M1 : distant metastases
Stage groupings
· stage I : T1 N0 M0
· stage II : T2 N0 M0
· stage III : Everything between II and IV
· stage IV : any one of : M1 or N2 or T4
Robson staging of renal cell carcinoma (RCC) is simple but has largely been replaced by theTNM system (see renal cell cancer staging article). Robson staging revolves around the relationship to Gerota's fascia, involvement of renal vein and regional nodes.
· stage 1 : limited to kidney
· stage 3
o 3a : renal vein involvement
o 3b : nodal involvement
o 3c : both 3a and 3b
· stage 4
o 4a : direct invasion of adjacent organs / structures
o 4b : distant metastases
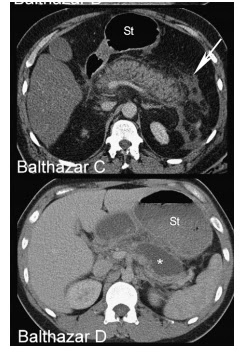
BALTHAZAR SCORING SYSTEM





Can accurately detect the disease in individuals with mutations in either PKD1 or PKD2 gene.
They determined that in families of unknown gene type
Presence of
Three or more kidney cysts is sufficient for establishing the diagnosis in individuals aged 15 to 39 years
Two or more cysts in each kidney is sufficient for individuals aged 40 to 59 years
Four or more cysts in each kidney is required for subjects ≥60 years.
Fewer than two kidney cysts in at-risk individuals aged ≥40 years is sufficient to exclude the disease.
For at-risk individuals aged 30 to 39 years, the absence of any kidney cysts provides almost certaint that the disease is not present.
Gallbladder polyp
· benign polyps : 95% of all polyps
o cholesterol polyps : > 50% of all polyps
o adenoma : ~ 30%, possibly premalignant
o inflammatory polyps
o adenomyomatosis
· malignant polyps : 5% of all polyps
o adenocarcinoma : ~ 90% of malignant polyps
o other rare entities including
§ metastases to gallbladder
§ squamous cell carcinoma
§ angiosarcoma
Benign vs malignant features of gallbladder polyps
Benign features
- size
- polyps that are less than 5 mm in size are almost always cholesterol polyps
- 5 - 10 mm polyps may warrant follow-up to ensure no interval growth
- morphology
- pedunculated
- number
- >50% of cholesterol polyps are multiple
- growth
- stable size
- CT / MRI enhancement
- similar to the rest of the gallbladder wall
- US features
- small echogenic focus / cluster of foci
- comet tail artefact (cholesterol polyp)
Malignant features
- size
- greater than 10 mm : 37-88% are malignant
- morphology
- sessile
- number
- solitary lesion
- growth
- interval increase in size
- CT / MRI enhancement
- greater than the normal gallbladder wall
Features of cholesterol polyp include:
- small size
- > 90% are less than 10 mm
- most are less than 5 mm
- echogenicity varies with size
- small polyps are echogenic but non-shadowing
- larger cholesterol polyps tend to be hypoechoic
- morphology
- small polyps are adherent to the wall and a smooth
- larger lesions tend to be pedunculated and granular in outline